I have read numerous papers on this issue and have to disagree with some aspects of some conlusions reached by students writing exam pieces. There is more to it and as a breeder we see in the bitch the structure of the dog and different worldwide Kennel Club requirements for being able to use a bitch for breeding. Some KCs wont allow breeding without a good hip score, others like the UK KC have no requirenments and that goes into the flow of the dog in the ring with some dogs according to some judges saying that dogs with tight hips don’t walk as well. Some overseas Kennel Clubs insist hips are scored and the bitch should have a good hip score, in over words there is little room for the hips to move and joints are deamed good. But. In a bitch where you have a more flexible skeletal movement and the rear legs can flex but then ask how tight is the muscles and how much restriction doesthat put on the vaginal area before birth.
When we have a litter we try and know what to expect before whelping as having breech puppies or non dilated vaginas can mean pups getting stuck and consequently injury and death. This has a medical name and can be seen better in written papers. Here is a link to Vet Folio https://www.vetfolio.com/learn/article/canine-dystocia-medical-and-surgical-management This same article has been on the Swiss corgi website for some time and this time written by Andrew Gendler, DVMa, Jeff D. Brourman, DVM, MS, DACVS, Kathleen E. Graf, DVM, DACVIM, WestVet Emergency and Specialty Center, Boise, Idaho.
Dystocia in Pembroke Welsh Corgis
Abstract
Dystocia is a common emergency in canine patients. The clinician must rapidly identify the stage of labor and determine whether veterinary attention is warranted. Physical examination, vaginal examination, abdominal radiography, abdominal ultrasonography, fetal heart rates, and intrauterine pressures assist the clinician in diagnosing and managing patients with dystocia. Oxytocin administration, intravenous fluids, and calcium gluconate are the mainstays of medical management; however, approximately 62% of dystocia cases require surgical intervention. Anesthetic protocols tailored to the unique physiology of the term bitch and neonate, along with timely intervention, may lower the overall dystocia puppy mortality rate of 22% and dam mortality rate of 1%.
Dystocia, the difficulty in passing the fetus through the pelvic canal, is a common small animal emergency. Significant disparity exists between the events of normal and abnormal canine parturition. Positive clinical outcomes can be expected only when the clinician has a thorough understanding and knowledge of normal canine parturition, the pathogenesis and underlying etiology of dystocia, the criteria for diagnosing dystocia, and the appropriate medical and surgical interventions.
Normal Parturition
The dam’s whelping date may be determined using breeding dates, time of luteinizing hormone (LH) peak, ovulation date, or the first day of diestrus. Gestation duration in the bitch is approximately 57 to 72 days (average: 65 days) when established using breeding dates.1,2 This period varies because the postcoital viability of canine sperm is at least 6 days and because the ovulation date may not have been identified using progesterone or LH assays.2 Parturition occurs 63 days after ovulation and 64 to 66 days after the LH peak. The gestation length after the first day of diestrus is 56 to 59 days,1 but this date is rarely known for dystocia patients. Okkens et al3 found that gestation duration is negatively correlated with litter size in litters of seven or fewer pups and that there is no difference in length of gestation between primiparous and multiparous bitches.Once the appropriate gestation time has passed, the complex cascade of events leading to delivery begins.
Understanding the neuroendocrine cascade of parturition assists the clinician in managing the dam and understanding the etiology of dystocia. The accepted neuroendocrine model of canine parturition is initiated by the fetus. The fetal hypothalamic-pituitary-adrenal axis is activated by fetal stress and leads to the secretion of fetal glucocorticoids.4-6 This increased glucocorticoid concentration stimulates maternal estrogen production, contributes to the synthesis and release of prostaglandins, and increases oxytocin receptors on the myometrium. Prostaglandins are luteolytic, contribute to the decline in circulating progesterone, remove the inhibition of myometrial contractility, and mediate the effects of oxytocin on the uterus.4 Maternal oxytocin is initially released from the hypothalamus in response to afferent stimulation of pressure receptors within the cervix and vagina. Relaxin hormone, produced by the ovary and placenta, assists fetal passage by allowing the interpubic ligament to elongate and the pubic bones to separate.4 The prolactin (lactation hormone) level, which increases gradually during gestation starting 21 to 28 days after ovulation,5 rises suddenly with the decline in the progesterone level.
Normal parturition is divided into three stages (Table 1) with predictable signs of forthcoming labor.4-6

Restless behavior, anorexia, and nesting may all be seen several days before parturition as well as during stage 1 of labor.5,6 Mammary gland turgidity, milk secretion, and relaxation of pelvic and abdominal musculature are described.4-6 A decline in rectal temperature below 99.7°F (37.6°C) has been cited as the most consistent change indicating that parturition will take place within the next 12 to 24 hours.5-7 This drop coincides with the decrease in the plasma progesterone level below 2 ng/ml. A recent study8 found no association between body temperature decline and impending parturition but did find a significant increase in body temperature 12 hours after the onset of parturition was identified. Limited conclusions may be drawn from this investigation owing to its small number of subjects. The authors suggested that direct measurement of progesterone decline and prostaglandin elevation is a more reliable indicator of parturition and that any elevation in the bitch’s temperature at the end of pregnancy without expulsion of fetuses could indicate dystocia.8
Each stage of labor has a predictable group of clinical signs and duration. Stage 1 labor begins with indiscernible uterine contractions and progressive cervical dilation. This stage lasts 6 to 12 hours, but primiparous bitches may persist for up to 24 hours. Behavior signs associated with stage 1 labor include nesting, panting, and restlessness. The second stage of labor is the active expulsion of the fetus from the birth canal; the visible abdominal straining matches the strong uterine contractions. Clear vaginal discharge, the allantoic fluid, is seen as stage 2 labor begins and precedes each puppy. The first fetus is normally delivered within 30 minutes of the start of stage 2 labor but may not be delivered for 2 to 4 hours due to weak or uncoordinated uterine contractions. Stage 2 labor should be complete within 12 to 24 hours, with a fetus produced every 0.5 to 4 hours. A recent case report9 described the delivery of a healthy puppy after a 34-hour interval between puppies and 37-hour duration of stage 2 labor—an interesting outlier within the dystocia patient population. Stage 3 labor is the expulsion of the placenta, which takes place 5 to 15 minutes after the delivery of the fetus. Multiple placentas may be passed after several puppies are delivered close together. It is not uncommon for the bitch to bite the amniotic and allantoic membranes, sever the umbilical cord, and ingest the placenta after parturition.4-6,10
Postpartum findings in the bitch may include mild fever, transient vomiting and diarrhea, and lochial discharge. Lochial discharge, produced by hemoglobin breakdown, is normal after parturition and is associated with uterine involution.6 The discharge is green to red-brown, odorless, and persists for up to 6 weeks.4-6,10
Criteria for Diagnosis of Dystocia
Veterinarians and their support staff are routinely confronted with phone calls and inquiries regarding canine parturition. The criteria in see Box.

have been reported4,5,7 as useful for advising owners when examination of the whelping bitch is appropriate. The criteria are intentionally stringent to facilitate earlier examination of the dam by veterinary personnel and reduce neonatal complications associated with prolonged dystocia.7
Pathogenesis of Canine Dystocia
Dystocia has conventionally been described as being of maternal or fetal origin. Maternal dystocia is encountered more frequently (60%11 to 75.3%12 of dystocia cases reviewed). The most common cause of maternal dystocia is uterine inertia, representing 40%11 to 72%12 of all dystocias attributed to the dam. Uterine inertia is the failure to expel a fetus from the uterus when no obstruction exists; it can be classified as primary or secondary. Complete primary uterine inertia occurs when stage 2 labor fails to start and no puppies are delivered. Partial primary uterine inertia is defined as initiation of normal labor but failure to deliver all puppies. Primary uterine inertia can develop because of litter size: either the litter is too small, or the myometrium is overstretched secondary to a large litter. More than 50% of studied bitches with complete primary inertia had three or fewer pups in their litter.12 Primary uterine inertia is also attributed to inherited predispositions, nutritional or neuroendocrine imbalance, age-related changes, nervous inhibition, and systemic disease.5,6 Secondary uterine inertia is the exhaustion of uterine musculature after contracting against an obstruction and has been reported as accounting for 3.2%12 to 12.6%11 of dystocias. Obstructions can include maternal changes or characteristics such as a narrow pelvis, congenital malformation, pelvic trauma, neoplasia or abscess, vaginal stricture, uterine torsion, uterine or vaginal prolapse, and vaginal hyperplasia.5,6
Fetal anatomic and orientation changes accounted for most reviewed cases of fetal dystocia (24.7%12 to 40%11 of dystocias). Oversized (6.6%12 to 13.7%11), malformed (1.6%12), or malpresented (15.4%12 to 15.8 %11) fetuses can cause dystocia, as can dead (1.1%12) or glucocorticoid-deficient fetuses. Puppies are delivered in cranial presentation 60% of the time; however, there is no predilection for dystocia based on delivery position.13 A combination of maternal and fetal factors may lead to the development of dystocia.
Several dog breeds are associated with an increased risk for dystocia. Scottish terriers and Boston terriers have inherited characteristics that predispose them to obstructive dystocia.14 Secondary uterine inertia occurs in Scottish terrier bitches with dorsoventral pelvic flattening and smaller vertical pelvic canal diameter.14 Boston terriers have similar pelvic measurements, but fetal oversize is a contributing factor to obstruction.14 The Chihuahua, dachshund, Pekingese, Yorkshire terrier, Pomeranian, and miniature poodle were the breeds most commonly represented in a retrospective study11 of 128 dystocia cases in the United States. Another study12 of 182 dystocia cases in Sweden did not find a significant breed disposition. Accurate identification of breed predispositions to dystocia has been limited by local breed popularity and failure of investigators to obtain a representative sample of the dystocia patient population.
Management of Abnormal Parturition
Initial evaluation of the dam requires an accurate history and thorough physical examination. Pertinent information includes breeding dates, ovulation date, vaginal cytology, and preovulatory LH peak date, when available, to establish a whelping date. An accurate history of the dam’s behavior for the previous 24 to 48 hours will help define the stage of labor and assist the clinician in deciding which interventions are indicated. Owners should also be questioned about the dam’s previous reproductive history, age, and breed and any treatments or manipulations performed before presentation.5″7 Standard historical information, such as current medications, past or chronic medical conditions or surgeries, adverse reactions to medications, and a systems review to check for signs of systemic disease, is important for case management.
Physical examination of the bitch should be efficient, yet thorough, and should cover all major body systems, with particular focus on the cardiovascular system and urogenital tract. Abdominal palpation is performed to check for the presence and position of pups, uterine contractions, and signs of abdominal pain, which may indicate uterine pathology.7 Palpation is not an accurate method of determining litter size.15 Mammary glands should be examined for the presence of milk and degree of development. Long hair around the vulva should be clipped and the skin cleaned in preparation for a vaginal examination. Sterile gloves are used during the vaginal examination, during which the clinician may detect a fetus, vaginal septa, masses, strictures, or pelvic abnormalities. Fetal presentation may also be determined.
Without vaginoscopy, cervical examination is impossible in most bitches, but vaginal vault diameter and muscular tone are described as possible indicators of cervical dilation.5,7 Anecdotal evidence suggests that a minimum of 1.5 x 1.5 inches of vaginal diameter is required to deliver the fetal head7 and that vaginal muscular tone may correlate with uterine tone.5 Vaginal examination also allows the clinician to characterize the dam’s vaginal discharge (Table 2).

The dorsal vaginal wall should be digitally stimulated (feathering) to see if strong abdominal contractions can be elicited (Ferguson reflex). Lack of response to the Ferguson reflex may indicate that the bitch is experiencing uterine inertia, is not in labor, or is exhibiting voluntary inhibition because of excessive stress and excitement.6
Abdominal imaging is important in the continued workup and management of the dam. Radiographs can detect mineralized fetal skeletons 43 to 54 days after breeding15 or 45 days after the LH peak.16 Fetal mineralization can be used to estimate gestation: the fetal pelvis, ribs, radius, and ulna appear on radiographs 11 days before parturition, and teeth appear 4 days before parturition.16 Abdominal radiographs are valuable in identifying malpositioned puppies and in providing an accurate fetal count4-7 (Figure 1) and are important to rule out the presence of an obstructive mass lesion (e.g., pelvic fracture, neoplasia).

Radiography is a poor modality to assess fetal viability because the typical changes denoting fetal death (intrafetal gas, collapse of the spinal column, and overlap of skull bones) do not appear until approximately 6 to 24 hours after fetal death.4-7,15
Abdominal ultrasonography has not proven useful in estimating gestational age at or around the time of parturition17,18; however, it is an excellent method of assessing fetal viability because it allows visualization of fetal movements and heart rates. An experienced ultrasonographer can also estimate fetal size by measuring fetal biparietal and thoracic diameters; these measurements can then be compared to the dam’s pelvic diameter on radiographs to determine oversize.19 Ultrasonographic signs of fetal death include lack of heartbeat or movement, increased echogenicity and decreased volume of fetal fluids, and increased gas in the fetal stomach.19 Fetal bradycardia, or heart rate below 150 to 200 bpm, can result from hypoxia and is an early indicator of fetal distress.7,19 Fetal bowel movements detected by ultrasonography can be another indicator of distress. Investigators identified a correlation between increased fetal bowel movements and severe fetal distress (defined as fetal heart rate <180).20 An experimental model of surgically induced fetal hypoxia in 12 bitches demonstrated that late deceleration of fetal heart rates was an early indicator of fetal hypoxia and decreased fetal blood pH.21
Survey blood work with priority given to packed cell volume and total protein, blood urea nitrogen, glucose, and calcium levels is beneficial to complete the patient assessment.
Medical Management of Dystocia
Medical management of the dam may be initiated before some of the above diagnostics are completed. Management includes digital or forcep fetal manipulation and the administration of medications to augment uterine contractions (see Box).
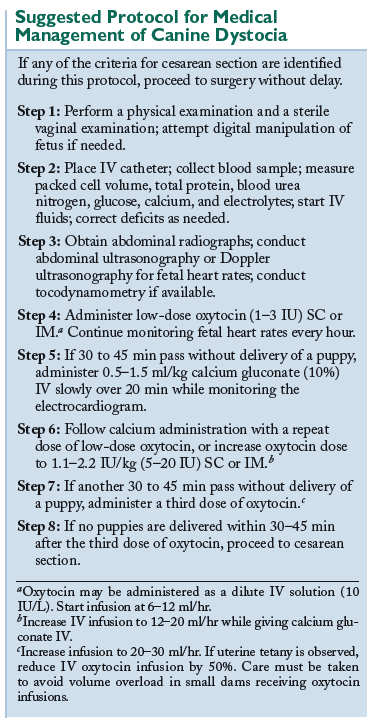
When a fetus is detected within the vaginal canal, the clinician may attempt to extract it. Fetal extraction should be accomplished using generous amounts of sterile, water-soluble lubricant and digital manipulation. Based on vaginal anatomy, the fetus should be gently pulled caudoventrally, with care not to exert excessive traction on the fetal limbs. The puppy’s shoulders or pelvis may be rotated into the dorsoventral plane of the dam’s pelvis to provide the greatest width for passage of the body. Use of instrumentation to manipulate and extract the fetus is possible but is not recommended due to the risk of fetal and maternal injury.
When maternal and fetal obstructions have been ruled out, the stimulation of uterine contractions may be initiated. This may be accomplished by having the owners walk the dam or by the clinician feathering the dam’s dorsal vaginal wall.22 Oxytocin administration is an effective technique to augment labor. While there has been little investigation into the optimum dose or route, the recommended dosage of oxytocin is 1.1 to 2.2 IU/kg IM or SC with a dose range between 5 and 20 IU q30min to effect.23,24 Concurrent administration of IV calcium gluconate (0.5 to 1.5 ml/kg of 10% solution) may augment oxytocin’s effect on myometrial contraction. Investigators have found that oxytocin-induced myometrial contractions are dependent on the influx of extracellular calcium.25 Lower doses of oxytocin (1 to 3 IU SC or IM) may stimulate uterine contractions while avoiding the possible negative effects of excessive oxytocin, which include uteroplacental blood flow interruptions and ineffective, tetanic uterine contractions.26
Administration of oxytocin as a dilute IV solution (10 IU of oxytocin per liter of isotonic crystalloid, 10 mU/ml) to effect at a slow drip rate is also reported.4 The limitations of this technique are based on the inability to accurately monitor the dam’s uterine contractions. Human obstetricians routinely use oxytocin as a continuous-rate infusion, with several protocols well described in the literature.27,28 Regardless of the method of oxytocin administration, the clinician should provide the dam with intravenous fluids to correct hydration, electrolyte, and blood glucose abnormalities. There is evidence in humans that mothers given higher rates of intravenous fluids have a shorter duration of labor and decreased need for oxytocin administration.28
An anxious dam that is voluntarily inhibiting uterine activity may present a special challenge. If stable, these patients may be placed in a quiet, dimly lit, comfortable room with their owners while their labor is managed (veterinary staff should check on the dam and owners every 15 to 20 minutes). If the clinician believes the dam is excessively agitated, low doses of a sedative, such as an opioid or a benzodiazepine, may be given to facilitate the labor process.
Intrapartum monitoring of the fetus and uterine activity allows the clinician to better medically manage labor and identify the need for early surgical intervention. Human medicine sets the standard for the monitoring of uterine activity and fetal physiologic variables. Current monitoring tools available to the veterinarian include B-mode ultrasonography, Doppler (fetal heart rate) ultrasonography, and tocodynamometry, which can detect changes in intrauterine pressure.29 Intrauterine pressure monitoring is currently only described for at-home use by breeders (WhelpWise system; Veterinary Perinatal Specialities, Wheat Ridge, CO), and its accuracy has yet to be critically evaluated.29 However, the concurrent use of Doppler ultrasonography and tocodynamometry would allow veterinarians to accurately identify the current stage of labor, adjust oxytocin and calcium therapy with acumen, and avoid the adverse effects of excessive oxytocin (uterine tetany, fetal hypoxia, and uterine rupture).29
The reported rate of dystocic dams whelping with medical management alone is approximately 30%.11,12 In one retrospective study,12 62.4% of bitches required cesarean section despite medical management for dystocia, and the total puppy mortality rate (regardless of intervention) was 22.3%. The duration of stage 2 labor has been shown to affect outcome. Gaudet11 found that the puppy mortality rate increased when the dam had been in stage 2 labor for longer than 6 hours before veterinary assistance was sought. Darvelid and Linde-Forsberg12 identified an increase in puppy mortality rates from 5.8% to 13.7% when the bitch had been in stage 2 labor for longer than 5 hours. These studies support the efficient and timely management of dystocia cases to reduce neonatal mortality rates.
Criteria for Cesarean Section

The Box lists the indications5-7 for an immediate cesarean section. The veterinary literature has yet to critically evaluate these indications, and further study in this area may elicit a more precise protocol to improve postoperative outcomes for the dam and puppies.
Surgical Management of Dystocia
Once the decision to perform a cesarean section has been reached, surgery should be performed in a timely manner. Owners should be counseled about the risks of surgery to the dam and neonates and asked whether they would like the dam spayed during the cesarean section. Abnormalities in the previously obtained blood work that remain after medical management should be addressed while preparing the patient for surgery. Intravenous fluids may be administered at the intraoperative rate (10 ml/kg/hr) during preparation for surgery to help improve intravascular volume, correct electrolyte shifts, and counter hypotension secondary to anesthesia.30 Efficient preparation of the abdomen (clip and aseptic scrub) is recommended before anesthesia to reduce the induction-to-delivery time and thus reduce neonatal mortality. Calm and gentle handling of the dam is also advocated to minimize excitement and catecholamine release, which decreases uterine blood flow and can contribute to fetal hypoxia.30
Based on the occurrence of supine hypotension syndrome in women, tilting the bitch 15° to 20° off midline has been suggested to prevent caudal vena cava compression by the gravid uterus during cesarean section. Investigators failed to identify any change in systemic arterial blood pressure regardless of position in small-, medium-,31 and large-breed bitches32 (up to 12.2 lb [27 kg]) and postulated that this was due to adequate collateral circulation and the bicornuate uterus.31 Dorsal recumbency is an acceptable position for the bitch during surgery.
Anesthetic Protocols
The unique physiology of the pregnant patient guides the clinician in selecting the most appropriate anesthetic protocol for both the dam and the fetus. Pregnant dams have decreased lung volume, decreased functional residual capacity, and increased oxygen consumption, which predispose them to arterial hemoglobin desaturation and lung atelectasis.33 They also demonstrate an increased sensitivity to inhalant anesthetics, increased plasma volume and cardiac output, and lower systemic blood pressures.33 Pregnant bitches also have reduced esophageal sphincter tone and increased intragastric pressure, which makes regurgitation more likely.33 Therefore, it is advised to oxygenate the dam before induction, administer intravenous fluids intraoperatively, and use a cuffed endotracheal tube. Because the fetus is subjected to any anesthetic agent administered to the dam, and because all drugs that cross the blood-brain barrier can cross the blood-placenta barrier,33 the clinician should administer as little anesthetic as possible. Additional recommendations include using drugs with a short duration of action, using drugs that are reversible, and minimizing the time the dam is exposed to inhalant anesthetics.33
Use of premedicants has been a controversial topic. Opioid (e.g., fentanyl) use is advocated over use of phenothiazines (i.e., acepromazine).33,34 Opioids provide sedation and analgesia and have advantages over acepromazine with their short duration of action, reversibility, and lack of identification as a risk factor for the neonate.33,34 Neonatal clearance of acepromazine is delayed because of poor hepatic metabolism; therefore, use of this agent should be avoided.34 If additional sedation of the dam is required, benzodiazepines can be considered. The use of an anticholinergic drug that crosses the placental barrier, such as atropine, may improve neonatal outcomes by increasing cardiac output.34
Accepted protocols for anesthetizing the pregnant bitch include epidurals, administration of propofol or a barbiturate, and mask induction, followed by inhalant anesthesia maintenance. Epidurals are routinely used in women to provide adequate analgesia for cesarean section with minimal effect on the neonate. Epidurals, using lidocaine alone or in combination with opioids, have been reported to produce the least respiratory and neurologic depression in puppies obtained through cesarean section35 and the best puppy survival rates.36 Canine epidural patients frequently require administration of additional narcotics, can suffer from hypotension, and may experience postoperative urine retention or hindlimb paresis.34
Propofol, a short-acting induction agent, has advantages over barbiturates based on its rapid hepatic metabolism and clearance. Barbiturate agents are more likely to lead to higher fetal mortality rates36,37 and greater reduction in compensatory neurologic reflexes present at birth35 compared with propofol. Survival rates are comparable between groups receiving propofol-isoflurane (89% of puppies alive at birth) and epidural analgesia (83% of puppies alive at birth), while the use of barbiturates had significantly fewer survivors (56% of puppies).36 Moon and Erb38 identified the use of thiobarbiturates, ketamine, and inhalant anesthesia as perioperative factors associated with decreased puppy vigor (vigor was defined as spontaneous breathing, vocalization, and movement at birth).
Halogenated agents, like isoflurane, make excellent maintenance anesthetics and provide uterine relaxation, which facilitates manipulation of the fetus during the cesarean section.30 Use of isoflurane was found to increase the odds of puppy vocalization at birth.38 Moon et al39 also showed favorable effects on neonatal survival rates with propofol and isoflurane in combination, but the difference was not statistically significant. Methoxyflurane was an inhalant associated with a decreased chance that all puppies would be alive at birth.39 The use of sevoflurane has not been identified as a perioperative risk factor reducing puppy vigor or mortality. Mask induction using inhalant agents may have the advantage of exposing the neonates to an anesthetic agent that can be cleared by simple respiration. This potential benefit must be weighed against the need for restraint and potential catecholamine release in the dam.30
Surgical Considerations
Cesarean section is required in 59% to 65% of bitches presenting for dystocia.11,12 The surgical technique to perform a cesarean section has been well described.40″42 The surgeon makes a ventral midline approach to the abdomen, taking care to avoid uterine or neonatal lacerations while incising the linea alba. The uterus should be isolated and packed off with surgical laparotomy sponges. A single incision is made in the body of the uterus, and all fetuses are manipulated to this incision for extraction. For each fetus, either the entire fetal sac and placenta is removed, or the fetal membranes are broken open and the umbilicus is ligated and divided before the puppy is transferred to an assistant. Once all neonates have been removed, the uterus should be palpated and visually inspected from cervix to ovaries. The uterine incision may be closed with absorbable suture and a single-layer suture pattern.
En-bloc ovariohysterectomy is an alternative cesarean section technique that rapidly removes the gravid uterus for an assistance team to extract and resuscitate all puppies outside of the operating room. Robbins and Mullen43 demonstrated no significant difference in neonatal survival rates for dogs delivered via ovariohysterectomy compared with rates for dogs delivered by traditional cesarean section.42 In this study,43 19 dams showed a mean decrease in total protein of 0.4 g/dl and in packed cell volume of 2% but did not exhibit decreased oncotic pressure or anemic packed cell volume.Traditional theory holds that ovariohysterectomy at the time of dystocia adds to the stress on the dam because of additional blood loss, fluid shifts, and prolonged anesthesia. One retrospective analysis11 found that dams that underwent ovariohysterectomy and hysterotomy had longer hospital stays and an increased incidence of postoperative complications than dams that underwent hysterotomy alone.
Routine postoperative care for the dam is indicated, including pain management, continued intravenous fluids, and heat support. When the dam is discharged, the owner should be counseled about common postpartum and postoperative complications, including normal serosanguineous vaginal discharge for 4 to 6 weeks, metritis, mastitis, eclampsia, incisional seroma, hematoma or abscess, and vomiting or diarrhea.
Management of the Neonate
Neonatal care must be prompt, attentive, and tailored to each patient based on the dam’s prior management and any congenital problems noted at birth. Resuscitation of the neonate requires the rapid clearance of fetal membranes and suctioning of the mouth and pharynx. Brisk rubbing with a warm towel is an excellent respiratory stimulant; if cyanosis is evident, the neonate may be provided supplemental flow-by oxygen or oxygen through a snug-fitting mask.44
Spontaneous breathing and vocalizing within 1 minute of birth have been identified as positive indicators of neonate survival.30 The adverse effects of inhalant anesthetics, benzodiazepines, and opioids administered to the dam may be evident in the neonate. Stimulating respiration increases neonatal ventilation and clearance of inhaled anesthetic gas; administering flumazenil 0.1 mg/kg IV antagonizes benzodiazepine-induced sedation; and naloxone, 1 drop sublingually, may be used to reverse opioid narcotization.45 Doxapram (Dopram, Fort Dodge) is a central nervous system stimulant routinely used in veterinary neonates. Current opinion cautions against its indiscriminate use because of a short duration of action, decreased effect on the hypoxic brain, and tendency to decrease cerebral blood flow.44,45 The act of swinging the newborn puppy to clear its airways is also discouraged to avoid accidental traumatic cerebral injury.
Adequate heat support (at least 90°F [32.2°C]) and umbilical care (cord ligated 1 to 2 cm from the abdomen) should be provided before reintroducing the puppies to the dam. All puppies should be examined for common congenital abnormalities, such as cleft palate, umbilical hernia, and atresia ani. The dam should be observed in the early postoperative period and the puppies returned to nurse when the dam is sternal and alert. The puppies should be bathed in amniotic fluid and returned to the dam with the placentas and membranes.46 Evidence demonstrates significantly improved newborn acceptance and prevention of newborn rejection when puppies are bathed in amniotic fluid before being presented to the dam.46
Outcomes
Significant canine neonatal mortality rates are reported regardless of the intervention provided. A large, multicenter prospective study47 to examine cesarean section mortality rates was conducted, with 3,908 puppies delivered from 808 dams. Puppies delivered by cesarean section had mortality rates of 8% at birth, 13% 2 hours later, and 20% at 7 days after parturition. Puppies born vaginally during dystocia had mortality rates of 14%, 17%, and 25%, respectively, at the same time intervals described above.47 Funkquist et al36 reported similar neonatal survival data after cesarean section but also identified a significant increase in mortality when some puppies had been born vaginally before cesarean section. This finding supports retrospective data11,12 that identified increased puppy mortality when stage 2 labor was prolonged and is in agreement with the cited overall dystocia puppy mortality rate of ~22%. Maternal mortality rates were reported to be 1% even after 58% of the cesarean sections were performed on an emergency basis.47
Conclusion
Accurate identification of dystocia and the patient’s stage of labor, improved use of maternal and fetal monitoring systems, and use of anesthesia tailored to the dam and fetus may help reduce the overall fetal mortality rate described in the veterinary literature.
